








































































































































































For several weeks, a 25-year-old man has been bothered by a pruritic rash on his hands. He has a history of allergies but is otherwise healthy. He owns 2 dogs.

For several weeks, a 25-year-old man has been bothered by a pruritic rash on his hands. He has a history of allergies but is otherwise healthy. He owns 2 dogs.

For 1 month, a 54-year-old woman has had an intensely pruritic eruption on her abdomen, arms, and anterior thighs. She has long-standing hypertension and type 2 diabetes mellitus, which are treated with an angiotensin-converting enzyme inhibitor/diuretic and an oral hypoglycemic agent.

This worsening rash developed after a 40-year-old man was treated with amoxicillin for an upper respiratory tract infection. When the rash started, the amoxicillin was discontinued and azithromycin was prescribed; however, the rash has persisted. The patient has no history of allergies or rashes. He takes no other medications.
Syphilis took Europe by storm at the end of the 15th century in what was to become a sweeping epidemic. Before 1495, it was unknown or perhaps was attributed to other disease processes, such as leprosy.

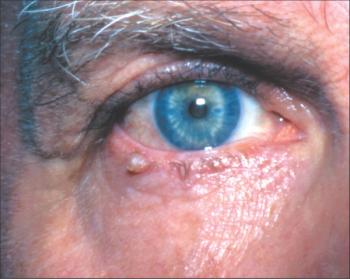
A 76-year-old man is seen because of redness below the right eye. Has long-standing “lazy eye” on the left, which is chronically deviated outward. Has lived in nursing home for some years due to self-care deficit from memory loss. No recent eye surgery, conjunctivitis, sinus infection, or periocular trauma.

This rash erupted on the upper body of a 58-year-old woman in late August. It was mildly pruritic and nontender. The patient had not started any new medications and was not taking photosensitizing drugs. She had Sjögren syndrome; the rest of her history was noncontributory. Subacute cutaneous lupus erythematosus (SCLE) was diagnosed. SCLE typically affects white women aged 30 to 40 years.1 It presents as nonindurated, nonscarring, erythematous plaques with or without a fine scale that may progress into a diffuse, widespread, papulosquamous or annular lesion with central hypopigmentation or telangiectasia.
A 44-year-old man seeks evaluation of itchy spots of 2 years’ duration on both forearms near the elbow. The condition failed to respond to topical corticosteroids prescribed by other physicians. Skin biopsy results were inconclusive; they showed only mild inflammation.
I applaud Dr Henry Schneiderman for his remarks in a recent “What’s Your Diagnosis?” column regarding the proper way to perform auscultation and percussion of the chest (CONSULTANT, October 2008, page 874). I am a family practitioner, and I examine my patients on their bare skin.

This lesion appeared on the left outer thigh of a 28-year-old man after he took amoxicillin. The antibiotic had been prescribed for an upper respiratory tract infection with fever. Two years earlier, a lesion had appeared in the same anatomical region after ingestion of amoxicillin. A skin biopsy of the current lesion confirmed the diagnosis.

An 89-year-old woman is seen because of a white area on the tongue. She has been hospitalized on a behavioral health unit for 2 weeks; 1 day ago, enoxaparin was begun for a new left leg deep venous thrombosis. Recent antibiotic therapy for a urinary tract infection; candidal vulvitis followed and was treated with topical clotrimazole. Has penicillin allergy.

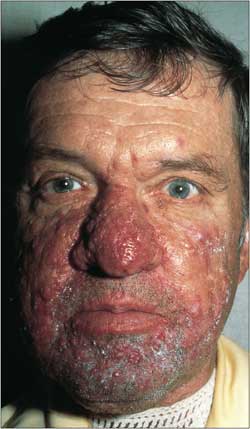
Cocaine abuse is associated with many dermatological manifestations, vasculitides, and infections. Consider this diagnosis in patients with unexplained chronic skin lesions, an ambiguous medical history, previous examinations that found no source of symptoms, labile affect, and delusional behavior.

These extensive, smooth, irregular masses of pigmented tissue on the earlobes of a 28-year-old woman are keloids. The patient had her ears pierced at age 6 years; the masses began to develop when she was about 9 to 10 years old. The right earlobe mass arose first and is larger. She had one other keloid of 1 cm on her chest that had developed after a scratch. She denied any other skin lacerations or incisions.
Methicillin-resistant Staphylococcus aureus (MRSA) was once considered a strictly nosocomial pathogen. Over the past decade, however, MRSA has emerged as a prominent cause of community-associated infections in both adults and children. Although community-associated MRSA strains occasionally cause severe invasive infections, they are most frequently isolated from patients with skin and soft tissue infections.
A previously healthy 16-year-old boy presents for evaluation of a slightly pruritic, nontender, generalized rash.
Untreated tinea versicolor has no grave sequelae. However, cutaneous dyschromia-hypopigmentation or hyperpigmentation-will persist without treatment (Figure).

For 25 years, a 74-year-old man had an intermittent, painful, and pruritic rash that caused cracking and erosions in the axillae and groin. It worsened with sweating and in the summer and also when clothing or skin rubbed against the eruption. The patient’s father, a paternal uncle, and all 3 of the patient’s daughters had a similar rash. Cetirizine and a combination of xipamide, bacitracin ointment, clotrimazole, and triamcinolone cream were prescribed to treat the rash.

For about 10 years, a 26-year-old man had recurring cystic lesions on his scalp that would periodically enlarge, shrink, and occasionally drain. One lesion had been excised by another physician, but it later recurred. The patient had been taking minocycline (100 mg) daily for this condition.

For a week, a 36-year-old Marine had clusters of localized papular lesions on the right forearm; he had no systemic symptoms. The patient had been inoculated 20 days earlier in the United States with the vaccinia virus (smallpox vaccine) to the ipsilateral shoulder just before deployment. He had no history of eczema, psoriasis, or drug allergies.

This finely papular, slightly raised lesion below the vermilion border of a 53-year-old man’s lip had been present for several months; it was asymptomatic. Six years earlier, the patient had a squamous cell carcinoma of the left lower leg excised. He worked outdoors on an offshore oil rig.

A biopsy of this asymptomatic lesion showed invasive squamous cell carcinoma without obvious perineural involvement. The lesion was excised with Mohs surgery, with good cosmetic outcome.

During a routine physical examination, flesh-colored papules were noted on a 36-year-old man’s elbows, knees, and interphalangeal joints. The patient reported that they had been present for a long time, were nonpruritic, and had remained the same color and size. He had not self-treated with any over-the-counter medications. His only other concern was acid reflux for which he regularly took antacids. He had no significant medical or surgical history and no medication allergy. He smoked 1 pack of cigarettes per day, drank alcohol socially, and consumed caffeine-containing drinks daily.
A 65-year-old man was concerned about a skin-colored papillary lesion on the right lateral lower eyelid along the eyelash line. It had been present for 1 week and was asymptomatic.

For 5 weeks, a 27-year-old man had a rash with painful fissures on his hands. For the past 2 weeks, he also had mildly pruritic red, scaly lesions on his trunk. He was otherwise healthy, had no allergies, and did not take any medications. The patient denied the use of tobacco, alcohol, and illicit drugs.

A 56-year-old man presented with pruritic, raised plaques with crusting and occasional weeping in tattoos he had acquired a few months earlier. The lesions were confined to the red and blue pigmented areas only, which suggested a contact dermatitis to the metal in the tattoo ink.
This pruritic rash appears to be a drug reaction to a cephalosporin. This class of drug often produces allergic reactions in the skin; this was quite an ordinary one, neither vasculitic nor urticarial. The mucosa was not affected, which ruled out Stevens-Johnson syndrome.