

Opinion|Videos|September 18, 2023
Infant Weight and Efficacy Outcomes of Nirsevimab for RSV
Author(s)Tina Q. Tan, MD, Flor M. Munoz, MD, MSc
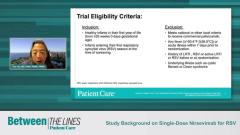
Experts discuss how infant weight related to efficacy outcomes of nirsevimab for Respiratory Syncytial Virus (RSV), providing their clinical expertise on why this may have occurred and what improvements can be made to mitigate these differences.
Advertisement
Episodes in this series








Transcript
Tina Tan, MD, FAAP, FIDSA, FPIDS: One other thing that was observed in this study was when they looked at infants under 5 [kg] and those 5 [kg] and over, they found that the relative risk reduction with nirsevimab was not as good as what was seen in infants who were 5 [kg] and over. And those who were under 5 [kg], the relative risk reduction for RSV was only around 52.4%, compared [with] 85.7% for those 5 [kg] and over. Can you comment on why that was a finding that came out of the study and why that might be?
Flor M. Munoz, MD, MSc: The authors of this paper do discuss that as well in the publication. That is one of the critical aspects, really understanding what dose is sufficient for babies, because we typically do a dosing based on weight. How much antibody you get, even though the half-life is prolonged, also would affect the duration of the effect of the monoclonal antibody, because obviously the higher the concentration, the longer the protection you would have. The discussion is it could be a matter of dosing and maybe optimizing the dose for the younger infants who are smaller, and being able to balance that higher dose with a good safety profile is going to be critical in this case. These are the babies who will have the highest risk, highest risk of exposures and also potentially the highest risk of developing more severe disease. The efficacy being lower in the very young might also reflect factors such as exposures, environment, the timing of registration, [and] the timing of circulation of the virus in the places where the study was done. I think that there could be multiple factors here, but it is an important point to keep in mind because, again, those are the highest risk, [infants] under 3 months. Once we start utilizing this preventive monoclonal antibody, I think it’s going to be very important to keep surveillance systems in place that we can [use to] assess the actual real-life efficacy, especially in the very young.
Transcript is AI-generated and edited for clarity.
Newsletter
Enhance your clinical practice with the Patient Care newsletter, offering the latest evidence-based guidelines, diagnostic insights, and treatment strategies for primary care physicians.
Advertisement
Related Content
Advertisement





Latest CME





























































































































Advertisement
Advertisement
Trending on Patient Care Online
1
First Oral Film Treatment for Erectile Dysfunction in Men Gains FDA Approval
2
Long-Term Data Support Sustained Bimekizumab Response in Hidradenitis Suppurativa
3
Weekly Dose Podcast: New Obesity Data, Insulin Guidance, and Mental Health Screening
4
Topline Phase 2 Data Show Roflumilast Cream Improves Atopic Dermatitis in Infants as Young as 3 Months
5