



































































































































For key facts and figures about musculoskeletal disorders, perhaps a surprise as the fourth leading diagnostic category in primary care, see the pages that follow.

For key facts and figures about musculoskeletal disorders, perhaps a surprise as the fourth leading diagnostic category in primary care, see the pages that follow.
What brings patients to your office-and not the specialty office down the street? Insights in this slideshow.
A new era in hepatitis C treatment began in May 2011, with approval of telaprevir and boceprevir. They are effective only for some patients, but new and better options are well on their way to the clinic.
Much like HIV/AIDS, RA is associated with a higher risk of cardiovascular disease and consequent death. How might inflammation add to the risk?

Joint deformity is far from the only concern in rheumatoid arthritis. The condition is associated with a variety of comorbidities and adverse events related to the medications used to prevent or treat symptoms, as these photos attest.
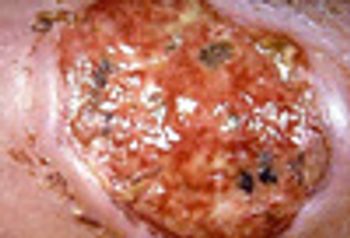
The location (pretibial surface) of this ulcer, its visibly rolled undermined border, and severe pain are all typical of pyoderma gangrenosum, which is typically associated with inflammatory bowel disease, rheumatoid arthritis, and hematologic malignancies.
Are persons with asthma at risk for other proinflammatory disorders? Yes, say researchers from the Mayo Clinic and Olmsted Medical Center in Rochester, Minn, who found that asthma is associated with the development of diabetes mellitus and coronary artery disease. However, there was no association between asthma and rheumatoid arthritis or inflammatory bowel disease.
More than half of patients with rheumatoid arthritis who were treated with a biologic discontinued treatment, and another 12% switched to at least 1 other biologic within a 2-year treatment period, according to a study led by Chureen Carter, PharmD, of Centocor Ortho Biotech Services.
As the number of biologic agents for rheumatoid arthritis (RA)-and rheumatologists’ use of these agents for RA and other rheumatological diseases-grows, getting coverage for RA treatment is taking an increasing investment of physicians’ staff time. However, the majority of respondents to a recent survey say it is an investment in patient care that is worth making.
ABSTRACT: Patients with rheumatoid arthritis (RA) often havepulmonary manifestations, such as interstitial lung disease.The most common cause of upper airway obstruction is cricoarytenoidarthritis. Patients often complain of a pharyngeal foreign-body sensation or hoarseness, but some present with severestridor. Bronchiolitis obliterans is characterized by a rapidonset of dyspnea and dry cough, with inspiratory rales andsqueaks on examination. This presentation, particularly in middle-aged women with seropositive disease, distinguishes bronchiolitisobliterans from other pulmonary manifestations ofRA. High-resolution CT may be more sensitive than pulmonaryfunction tests for detecting small-airways disease, and it frequentlyshows moderate to severe air trapping on expiratoryimages. (J Respir Dis. 2008;29(8):318-324)
We describe a case of sulfasalazine-induced pneumonitis ina complex medical patient.This case illustrates the potentialfor drug-induced pulmonarydisease and the vigilanceneeded in evaluating patientswith subacute respiratory decompensation.Proper recognitionand treatment mostlikely prevented the progressionof acute respiratory failureand, possibly, irreversiblelung injury or death.
ABSTRACT: Pulmonary manifestations, such as pleural effusions,interstitial lung disease (ILD), and rheumatoid nodules, arecommon in patients with rheumatoid arthritis (RA). For thosewith pleural effusions, diagnostic thoracentesis is usually necessaryto rule out other causes. Larger effusions that cause dyspneamay require therapeutic thoracentesis or other interventions.The presentation of ILD is characterized by graduallyprogressive dyspnea on exertion and cough. An isolated decrementin carbon monoxide–diffusing capacity is often the earliestabnormality seen on pulmonary function testing. HighresolutionCT is an important tool for detecting ILD; commonfindings include ground-glass opacities and reticulation. It isimportant to keep in mind that in RA-associated ILD, morethan one pathological process-often several-may be seen inthe same patient. (J Respir Dis. 2008;29(7):274-280)
Specialty medications constitute the fastest-growing segment of drug spending under the pharmacy benefit. This study evaluated the impact of a specialty pharmacy prior authorization (PA) program on prescription drug costs for biologic response modifiers (BRMs) used in the treatment of persons with rheumatoid arthritis, juvenile rheumatoid arthritis, Crohn disease, ankylosing spondylitis, psoriatic arthritis, psoriasis, and other spondyloarthropathies. A retrospective, case-control, one-to-one matching approach based on patient age, sex, and client characteristics was used. Case clients were enrolled in the specialty pharmacy PA program from January 1 through December 31, 2005. The control group consisted of clients who were not enrolled in the program during this time. The average costs per eligible member per month (PMPM), for the total, plan, and member were $1.32, $1.29, and $0.03, respectively, in the case group, and $1.44, $1.41, and $0.03, respectively, in the control group. Clients who implemented the specialty pharmacy PA program for BRMs saved an estimated total cost of $0.12 PMPM. Implementing a specialty pharmacy PA program reduced BRM costs. (Drug Benefit Trends. 2008;20:26-31)
BALTIMORE -- Patients with rheumatoid arthritis who meditated were measurably less stressed after six months than those given standard care, but the disease was no better, said investigators here.
LEIDEN, The Netherlands -- At least some cases of rheumatoid arthritis appear to be set in motion by mutations in two immunity-related genes, leading to increased susceptibility and severity of the disease.
PITTSBURGH -- The risk of developing diabetes decreased 38% among rheumatoid arthritis patients taking the antimalarial drug hydroxychloroquine (Plaqueril), according to a preliminary study.
BARCELONA, Spain -- Ofatumumab (HuMax-CD20), an investigational fully human antibody, appears to be safe and effective for rheumatoid arthritis, researchers said here.
BARCELONA, Spain -- Rheumatoid arthritis responds more quickly to certolizumab pegol (Cimzia) than to other tumor necrosis factor-a inhibitors, researchers have found.
VIENNA -- Three drugs, two approved and one in the pipeline, are improving care for patients with severe rheumatoid arthritis (RA), according to clinicians here.
A prediction model and simple scoring form developed by Dutch rheumatologists can help physicians determine which early-arthritis patients are most likely to develop rheumatoid arthritis and should therefore receive prompt, aggressive treatment.
LEIDEN, The Netherlands -- For early rheumatoid arthritis, aggressive combination therapy can slow progression to joint damage, investigators here found.
SYDNEY, Australia -- The swollen and twisted joints in the hands and feet from rheumatoid arthritis are associated with depression in patients who become unhappy with their physical appearance, researchers here said.
MANCHESTER, England -- Patients with inflammatory polyarthritis, often a precursor to rheumatoid arthritis, are 40% more likely than the general population to die of cancer, according to a prospective cohort study.
LIVERPOOL, England -- Low-dose glucocorticoid agents given along with standard disease-modifying drugs reduced the progression of early rheumatoid arthritis for up to two years, Cochrane reviewers reported.
US researchers recently reported initial phase 1 results from 2 vaccine candidates that successfully produced immune responses in healthy uninfected adults (Gibian JJ. United Press International. November 16, 2006). Eventually, the approach may be used to protect against HIV infection. Barney Graham of the NIH Vaccine Research Center and colleagues performed the tests (Graham BS, Koup RA, Roderer M, et al. J Infect Dis. 2006;194:1650-1660; Catanzaro AT, Koup RA, Roderer M, et al. J Infect Dis. 2006;194:1638-1649).