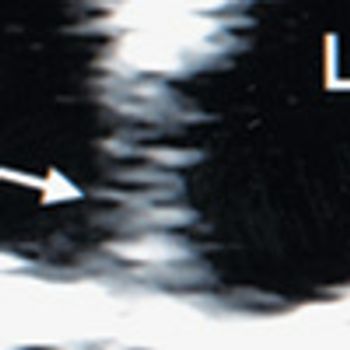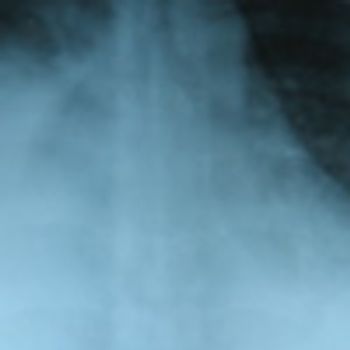
For 4 days, a 34-year-old pregnant woman had dyspnea and right-sided chest pain. She denied fever, chills, sweats, cough, lower extremity pain, and edema. Surgical and social histories were unremarkable. She was taking progesterone and clomiphene citrate for the past 6 months for assisted reproduction.