
Here: strategies for making the exam more comfortable and efficient, and tips for using topical anesthetics, removing earwax, extracting a plantar foreign body, and approaching the Dx of appendicitis.
Brady Pregerson, MD
Advertisement
Dr Pregerson's podcast EM Logic focuses on pitfalls in emergency medicine such as confusing a cause with a coincidence, being falsely reassured by false negative tests, or getting burned by illogical assumptions.
We hope to improve the care you provide your patients and keep you from being an honored guest at your department’s next peer review meeting.
The podcast can be heard by clicking here or searching “EM Logic” on Apple podcast or “Pregerson” on Spotify.
Dr Pregerson has been practicing emergency medicine since 2000, lecturing and writing about medical topics since 2004, and has reviewed more than 180 malpractice cases since 2008. He is the author of 3 EM pocket references, the creator of EMresource.org and EM1minuteconsult.com, and the author of the EMN column BradyCardia
If you would like to be considered as a guest on a future episode, contact Dr. Pregerson at [email protected].
Articles by Brady Pregerson, MD
The “take home” from this presentation: be cautious with inappropriate use of drugs with or without black box warnings, but maintain a healthy skepticism about some of these warnings. Cases in point: droperidol, antidepressants, clindamycin.
ECG findings that are specific for high-grade stenosis of the proximal left anterior descending (LAD) coronary artery.
Epigastric pain after meals occurs in the absence of physical or laboratory abnormalities in a 66-year-old woman slated for surgery.
Pulmonary embolism was the diagnosis in these 3 women, each of whom presented with positional right flank pain.
Three women-all of whom presented with positional right flank pain-- all had the same final diagnosis. What do you think it was?
Ramsay Hunt syndrome is a peripheral facial neuropathy that causes unilateral lower motor neuron pattern facial weakness. It is associated with a painful erythematous vesicular rash of the ear or nearby areas and/or oropharynx.

To what diagnosis does this painful swollen ear point in an HIV-positive man?
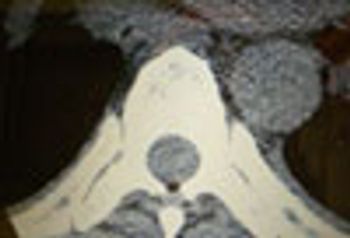
An obese woman in her thirties with a history of fibromyalgia syndrome, depression, polycystic ovarian syndrome, and diabetes mellitus presents to her local emergency department with 1 week of gradually worsening midline back pain.
An obese woman in her thirties with a history of fibromyalgia syndrome, depression, polycystic ovarian syndrome, and diabetes mellitus presents to her local emergency department with 1 week of gradually worsening midline back pain. What do these images show?
This patient had unilateral petechiae on the dorsum of the left foot. If the petechiae were symmetric, the first condition on the differential diagnosis would be thrombocytopenia. Here, though, the platelet count was normal. The patient also had a duplex of both the arterial and venous systems that showed complete thrombosis of both the arterial AND venous systems.

The patient has a stage 1 decubitus ulcer on her left heel. Both feet are cool but are the same temperature. Distal pulses are palpable but weak on the good foot; they are not palpable on the left and can only be heard faintly with a handheld Doppler. You note unilateral petechiae on the dorsum of the left foot.

The patient had been having slurred speech and trouble swallowing and chewing. He had been using his hand to hold his jaw closed and to push his jaw up to help him chew.
The patient, a 70-year-old man, has been having difficulty chewing and swallowing has been using his hand to hold his jaw closed while he eats; otherwise, his jaw hangs open. His speech is slightly slurred.
Most cases of “pink eye” are caused by infectious, or occasionally allergic, conjunctivitis. Occasionally, however, a rare and more serious condition-such as a corneal ulcer or iritis-may masquerade as conjunctivitis, as in this patient.

Look closely at this image. Does this look like conjunctivitis. . . or something else?
The key diagnostic considerations hypokalemia, periodic paralysis, and ischemia should lead the assessment of a patient with acute generalized weakness.

Vertebral artery dissection may be misdiagnosed as post-concussive syndrome, stroke, or TIA, based on neurologic symptoms. Always consider after neck trauma.

What is causing this clubbing of the fingernails, and what is it called?

A woman in her 20’s presents for care after 9 days of sore throat and subjective fevers followed by neck stiffness that developed over the last 2 to 3 days. The pain is exacerbated by swallowing and any neck motion. She has had sore throats before, but never this bad or this long and never that made her neck stiff.
For 3 days, a 47-year-old woman had a painful red swelling on her finger.The patient--a cellist--had tried to lance the lesion at home, but itprogressively worsened and was now “throbbing.” She denied fever andnail biting.
Advertisement
Advertisement
Advertisement
Trending on Patient Care Online
1
Understanding Wearables and Sleep Quality in Chronic Sleep Disorders, With Leanne Kaye, PhD, MPH
2
Elinzanetant Improves Sleep Independent of Hot Flash Reduction in Menopause
3
New and Emerging Tools for Managing Menopausal Sleep Disturbance, With Fiona Baker, PhD
4
Sleep Impairment as a Modifiable Dementia Driver, With Bryce Mander, PhD
5