



























































































































































































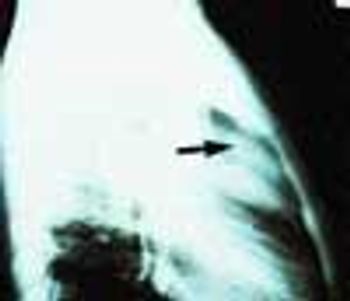
A 72-year-old woman who had fallen and injured the left side of her chest came to the emergency department complaining of pain in that area. She was physically stable and not short of breath. A soft systolic murmur was heard over the left precordium; the lungs were clear. A posteroanterior chest film showed no rib fracture but it did show an enlarged heart and a large, calcified ventricular aneurysm.