





























































































































As many as half of patients who are evaluated for abdominal pain do not receive a precise diagnosis. And for about half of those who are given a diagnosis, the diagnosis is wrong. In this article, I will use actual cases (not "textbook" examples) to illustrate an approach to abdominal pain that begins with a careful differential diagnosis. I also offer some general guidelines for evaluating patients.
Sleep Disorders
Latest News
Advertisement
CME Content
Advertisement
A systematic approach to the patient with resistant hypertension is both cost-effective and rewarding because the evaluation will probably reveal the cause. Initial considerations include lack of adherence, inappropriate treatment, drug-drug interactions, volume overload, and white-coat hypertension.
Recently, the National Guideline Clearinghouse compared smoking cessation recommendations from the Public Health Service, the University of Michigan Health System, the Singapore Ministry of Health, the New Zealand Guidelines Group, and the US Preventive Services Task Force. Highlights of guidelines from the US groups are presented here.
In patients with underlying disease, a preoperative evaluation and targeted perioperative management strategies can minimize surgical complications and maximize healing. This article focuses on how to identify surgery patients at risk for complications caused by diabetes, chronic obstructive pulmonary disease (COPD), and other medical conditions; I also describe strategies to minimize such risk.
Traumatic brain injury may occur without visible head injury; it manifests as confusion, focal neurologic abnormalities, an altered level of consciousness, or subtle changes on neuropsychological testing. The initial evaluation includes assessment of the patient's airway and respiratory, circulatory, and neurologic status.
Abstract: Pulmonary function tests, such as the measurement of forced expiratory volume in 1 second (FEV1) and peak expiratory flow (PEF), provide an objective, standardized, and quantifiable method of patient assessment and can be essential in the evaluation of asthma. However, FEV1 and PEF are relatively insensitive for detecting changes in persons with good baseline pulmonary function, and they do not directly measure worsening airway inflammation. One way to deal with the shortcomings of these tests is to include multiple outcomes assessment. Evaluating patient-oriented variables, such as symptoms, need for rescue medication, nocturnal awakenings, and unscheduled medical care visits, can detect clinically relevant changes that pulmonary function tests do not identify. Composite outcomes provide a more comprehensive approach to patient follow-up. For example, a patient who is considered to be a "nonresponder" to a given therapy on the basis of pulmonary function criteria might, in fact, be responding favorably according to assessment of composite outcomes. Two patient-centric tools for measuring outcome are the asthma control questionnaire and the asthma control test.
Abstract: The coexistence of asthma and obstructive sleep apnea (OSA) in a given patient presents a number of diagnostic and treatment challenges. Although the relationship between these 2 diseases is complex, it is clear that risk factors such as obesity, rhinosinusitis, and gastroesophageal reflux disease (GERD) can complicate both asthma and OSA. In the evaluation of a patient with poorly controlled asthma, it is important to consider the possibility of OSA. The most obvious clues are daytime sleepiness and snoring, but the definitive diagnosis is made by polysomnography. Management of OSA may include weight loss and continuous positive airway pressure (CPAP). Surgical intervention, such as uvulopalatopharyngoplasty, may be an option for patients who cannot tolerate CPAP. Management may include specific therapies directed at GERD or upper airway disease as well as modification of the patient's asthma regimen. (J Respir Dis. 2005;26(10):423-435)
An 87-year-old woman who recently moved to an assisted living facility from her home is seen for evaluation of facial edema and erythema after a bee or wasp sting sustained 2 days earlier. Patient denies pain, pruritus, or visual changes. She took one dose of diphenhydramine shortly after the event and has noticed that the edema, which affected primarily the right side of the face, near the sting, has improved.
The metabolic syndrome represents a clustering of conditions and/or risk factors that lead to an increased incidence of type 2 diabetes mellitus and cardiovascular disease. These conditions include abdominal obesity, dyslipidemia, hypertension, insulin resistance, and a proinflammatory state.

An 87-year-old woman who recently moved to an assisted living facility from her home is seen for evaluation of facial edema and erythema after a bee or wasp sting sustained 2 days earlier. Patient denies pain, pruritus, or visual changes.

A 12-year-old boy with a history of atopy complained of pruritus and severe dryness of the hands. Over-the-counter moisturizers failed to resolve the condition. The patient did not wash his hands frequently and had no hobbies that exposed him to environmental irritants or allergens.

An otherwise healthy 4-year-old boy was brought for evaluation of a mildly pruritic rash, which had been present for approximately 8 months. The developmental history of the eruption was equivocal, and the child's mother reported no aggravating or ameliorating factors.
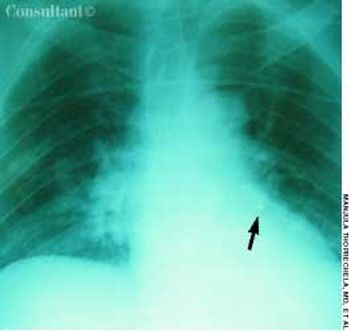
For 1 month, an 82-year-old woman had had episodes of coughing. Chronic bronchitis had been diagnosed; however, antibiotics and bronchodilators failed to control symptoms.
An 85-year-old white woman was brought to the emergency department (ED) with acute, severe left posterolateral chest wall pain of several hours' duration. The nonradiating pain was accompanied by shortness of breath. She denied palpitations, diaphoresis, syncope, or dizziness.

The extent of mucosal or transmural intestinal necrosis varies. Pneumatosis progresses from the submucosa through the muscular layer to the subserosa. The distal ileum and proximal colon are most frequently involved.

This newborn has Cornelia de Lange syndrome, a disorder characterized by prenatal growth retardation (this child weighed 2240 g at birth and measured 46 cm in length), microbrachycephaly, bushy eyebrows, long eyelashes, short neck, low posterior hair line, depressed nasal bridge, anteverted nares, long philtrum, thin upper lip, downturned corners of mouth, micrognathia, a single umbilical artery, phocomelia, micromelia, and oligodactyly.

This neonate was born with a high arched and cleft palate and a small jaw-the result of Pierre Robin syndrome, an autosomal recessive disorder also characterized by micrognathia and pseudomacroglossia.

This 20-month-old girl was born to a 28-year-old mother at 38 weeks' gestation. The pregnancy was uncomplicated, and vaginal delivery was normal. The infant sat with support at 10 months of age, sat without support at 12 months, crawled at 13 months, and walked at 18 months. She had not yet begun to talk at 20 months. The child was noted to have frequent laughing episodes and often made flapping movements with her hands.

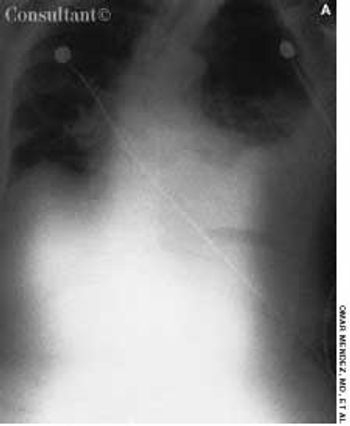
An obese 61-year-old man who had chronic obstructive pulmonary disease and sleep apnea heard a “pop” in his stomach while lifting a heavy weight; severe abdominal pain followed. He was short of breath the next morning, and his physician empirically prescribed cephalexin.
A 67-year-old woman was referred for evaluation of exertional dyspnea, with multiple episodes of fever, cough, and pneumonia. She had a long history of cough with sputum and had been admitted several times for exacerbations of chronic obstructive pulmonary disease and pneumonia. She received maintenance therapy with an ipratropium and albuterol combination, fluticasone, and salmeterol, but she continued to experience exertional dyspnea, with an average of 5 or 6 exacerbations and 2 hospital admissions a year.
56-year-old woman presents for evaluation of several syncopal episodes that occurred during the past 2 weeks. These episodes were associated with various activities--eating while seated, walking slowly, and standing upright--and rendered her briefly unconscious.
A 55-year-old man complains of fatigue. Although he sleeps 8 hours every night, he has to push himself to perform his usual daily activities. He has also experienced loss of libido and episodic impotence, which he ascribes to the fatigue.
Advances in the understanding of multiple sclerosis (MS) have translated into aggressive treatment regimens that enhance patients' quality of life. In this article, we discuss the therapeutic options, especially treatments that are directed toward the underlying immunologic mechanisms of the disease. Because of its direct effect on quality of life, aggressive management of symptoms is emphasized.
How to lessen insomnia during a sleep study.
An 82-year-old woman complains that for the past 6 months, she has "not felt like herself." Previously, she was very active and energetic; in fact, 9 months earlier, she had vacationed in Hawaii. It now takes all of her energy just to get out of bed.
Advertisement
Advertisement
Trending on Patient Care Online
1
Weekly Dose Podcast: New Obesity Data, Insulin Guidance, and Mental Health Screening
2
First Oral Film Treatment for Erectile Dysfunction in Men Gains FDA Approval
3
Topline Phase 2 Data Show Roflumilast Cream Improves Atopic Dermatitis in Infants as Young as 3 Months
4
Long-Term Data Support Sustained Bimekizumab Response in Hidradenitis Suppurativa
5