






















































































































































































































Low-potency corticosteroids had not resolved a rash of several month's duration on the buttocks of a 2-year-old girl.

Low-potency corticosteroids had not resolved a rash of several month's duration on the buttocks of a 2-year-old girl.
A 6-year-old girl with mental retardation was seen for a physical examination. She was being followed by a neurologist for seizures that began in her first year of life. She had no acute health problems.

Consultation was sought for diagnosis of the concentric rings of erythema and scaling that appeared on one side of a 42-year-old woman's face. The patient had used a moderately potent topical corticosteroid that had been prescribed for a facial "rash."

Several hours after returning from a walk in tall grass, a 9-year-old boy began to complain about intense itching around his waist, lower back, and upper arms. Wheals developed on these areas.

For 2 months, an asymptomatic rash had been present on the upper arms of a 16-year-old boy of normal weight. The rash, as seen on the patient's right arm, consisted of abundant fine papules. He had no other lesions.

Each spring for the past 3 years, this boy has complained of an itchy ear rash. The dull red edematous papules develop on the outer portion of the helix, and the rash heals promptly after 2 weeks.

This asymptomatic pigmented lesion on the left posterior jaw of a 52-year-old man had been present for 6 years, with no evidence of recent change. At the patient's request, the lesion was excised.

HIV infection was diagnosed in a 34-year-old man 3 years before he was hospitalized. The patient had a 2-week history of nausea; vomiting; and diffuse, intermittent, poorly localized abdominal pain. He had received radiotherapy and chemotherapy for Kaposi's sarcoma (KS) of the upper and lower extremities, which had been diagnosed 8 months earlier.

A male infant was born to a 29-year-old woman (gravida 3, para 2), following an uncomplicated pregnancy and normal vaginal delivery. At birth, a brownish 1-cm nodule was noted on the right side of the upper abdomen. The infant was otherwise healthy.

A 3-mm long, double-tipped, polypoid lesion appeared just anterior to the anus on an 8-month-old girl 2 days earlier. The lesion was excised in the office: a local anesthetic was administered, and the base was lightly electrodesiccated. Antibiotic ointment was applied until the area healed. Pathologic findings identified an infantile perianal pyramidal protrusion.

A 16-year-old boy removed a small sliver of wood from the palm of his hand with a pocket knife. However, the fledgling “surgeon” created a small puncture wound during this operation. Over the next month, a small, moist, friable papule grew at the site.

A 19-year-old man was admitted to the hospital with malaise, fatigue, and intermittent fever (temperature of 38°C [100.4°F]) for the last 2 weeks. Physical examination revealed scarce purpuric lesions over the lower extremities; a pericardial friction rub was audible over the precordium when the patient was supine and seated, and the spleen was remarkably enlarged.
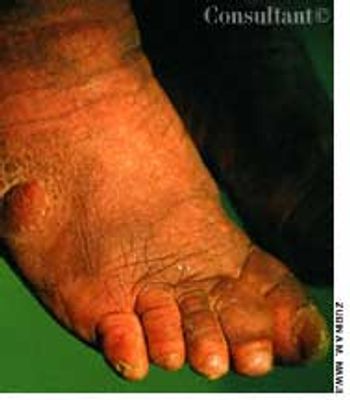
A 60-year-old white man was evaluated for dyspnea on exertion. Hepatomegaly and abnormal skin pigmentation were noted, particularly in the upper extremities.

A 49-year-old man was concerned about a right flexor forearm lesion that had been increasing in size for 6 weeks. The light pink, well-demarcated, 5-cm, circular lesion featured slight peripheral elevation with ulceration, crusting, and a relatively clear central area. A culture of material from the lesion was negative for fungi. A potassium hydroxide evaluation was not performed.

A 30-year-old woman had an extensive psychiatric history of anxiety and depression. She was concerned that the numerous lesions on her body might be signs of possible infection or infestation. The patient was undergoing treatment for multiple addictions to drugs, primarily methamphetamine (“crank”).
The persistent effects of Graves disease were evident in a 48-year-old woman who had recently emigrated from Haiti to the United States. Thyrotoxicosis had developed several years before she sought treatment in her native country. The patient's obstructive goiter was removed and treatment with thyroxine was begun.

A 6-year-old boy had a nonpruritic rash on his back for 10 days. There was no associated fever. The child's mother had placed a bandage over the lesions to prevent transmission to her other children.

Levofloxacin, 500 mg/d, had been prescribed for a 74-year-old woman who had a urinary tract infection. The patient had type 2 diabetes and hypertension. She was allergic to sulfa drugs.

This rash, which covered a 68-year-old woman's body, was noted to have worsened during the past 2 months. A cephalosporin antibiotic had failed to clear the condition. The patient, a nursing home resident, suffered from emphysema, asthma, and heart disease. She had been receiving oxygen therapy and prednisone for 1 year.

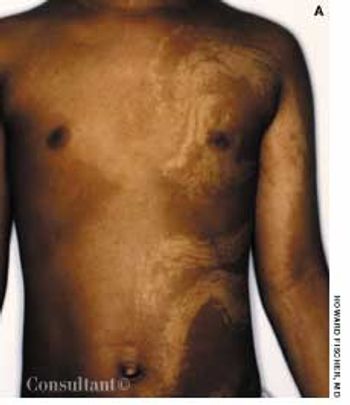
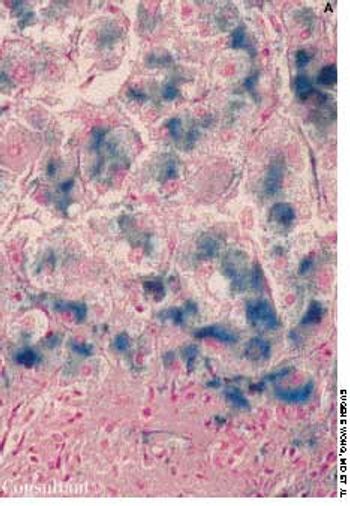
A 45-year-old African American man requested treatment of “keloids” that had developed 18 months earlier. The patient also complained of dyspnea and exertion; there was no history of trauma.

A brownish red, reticulate rash had persisted on the thighs of a 53-year-old man for about 15 years. For the past 20 years, he had applied-daily and for extended periods-a hot water bottle on his legs for soreness following exercise.
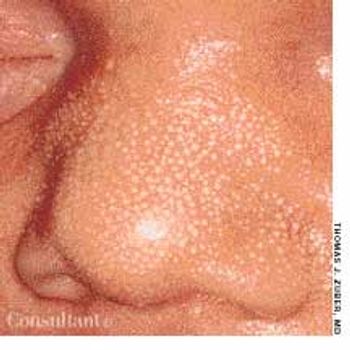
The mother of this 8-day-old newborn was concerned about the multiple white lesions scattered over the baby's face. Most of the tiny spots were clustered on the nose.

A 27-year-old man from Iraq presented with a painful lesion on the left lateral aspect of his tongue of 2 weeks' duration. Genital ulcers or skin lesions were not present. The patient also complained of a low-grade fever, weight loss, and occasional episodes of left eye pain during the past several months. He denied any significant past medical history, allergies, and the use of medications or illicit drugs.

The appearance of a wound on the hand of a 102-year-old man concerned his nursing home's staff. Several months earlier, the patient had had a squamous cell carcinoma removed from the wound site and had undergone subsequent radiotherapy. A nonhealing skin ulcer developed at the site; a skin graft was performed.

A 62-year-old man consulted his physician hoping to confirm his suspicion that this lesion was benign and caused by skin friction from his watch. The 0.75-cm, purplish red, raised, rounded, dome-shaped mass with a keratin-filled crater at its top was on the patient's left distal extensor forearm. The lesion had developed within 3 weeks.